Signs look promising that the United States will maintain its vital place as the world’s leader in combating HIV in poorer nations, notwithstanding a long-stagnated budget. In September, the U.S. State Department issued a document, signed by Secretary of State Rex W. Tillerson, sketching out the plans through 2020 for the U.S. President’s Emergency Plan for AIDS Relief. And while PEPFAR’s precise 2018 budget remains up in the air, Congress appears positioned to rebuff President Donald Trump’s springtime request for a devastating cut to the program, which is the crown jewel of President George W. Bush’s foreign policy legacy.
Long on vision but short on specifics, the State Department document has at least assuaged festering concerns among HIV advocates that Trump’s team was planning to scrap PEPFAR work in all but 13 hard-hit nations. The agency will continue to operate in more than 50 nations but focus its efforts on a baker’s dozen of hard-hit countries—Botswana, Ivory Coast, Haiti, Kenya, Lesotho, Malawi, Namibia, Rwanda, Swaziland, Tanzania, Uganda, Zambia and Zimbabwe—with the goal of achieving control of 10 of their epidemics by the outset of the next decade.
Epidemic control, by PEPFAR’s chosen definition, occurs when the annual number of new HIV infections drops below the rate of death from any cause among the national HIV population. When more people die than become infected, the size of a nation’s epidemic begins to contract.
The results of highly reliable, country-wide surveys of six sub-Saharan African nations released during the past 10 months suggest that for at least a few countries, the ambitious outcome of a controlled epidemic no longer amounts to a mere aspirational target. A massive drive to increase HIV diagnosis and successful treatment rates in hard-hit nations has a handful of countries already poised to hit a key tipping point: getting 73 percent of their HIV populations on successful ARV treatment, a milestone that Joint United Nations Programme on HIV/AIDS (UNAIDS) modeling predicts will ultimately lead to HIV’s elimination as a major public health threat in any particular country by 2030.

The gap between the annual rate of new HIV infections and AIDS-related deaths in the 13 nations PEPFAR has chosen to focus on.PEPFAR
To set them on a course to this milestone, UNAIDS has called upon all nations to get 90 percent of their HIV populations diagnosed, 90 percent of that group on antiretroviral (ARV) treatment and 90 percent of that group virally suppressed by 2020. Currently, of an estimated 36.7 million people living with HIV worldwide, 53 percent are on ARVs and 44 percent have an undetectable viral load.
The key to sending HIV infection rates tumbling is the awesome power of ARVs to both treat the virus and prevent its spread. Evidence from three major trials has led a wide network of experts, including the Centers for Disease Control and Prevention (CDC), to conclude that when an individual has an undetectable viral load thanks to ARV treatment, the risk that he or she will transmit HIV through condomless sex is effectively zero.
Attempting to read the tea leaves in the new PEPFAR plans, advocates have been heartened that the U.S. government has explicitly pledged to keep providing ARVs to those already receiving them through the agency’s work. Furthermore, the agency has made clear that it intends to drive up national viral suppression rates through expanded ARV treatment in the 13 priority nations. But advocates remain concerned that the United States may cap treatment levels in the remaining countries in which PEPFAR operates, since the agency has not explicitly pledged to treat more people in those nations. The agency has, however, said it will ramp up services to orphans and vulnerable children affected by the AIDS-related death of a caregiver.
David Paltiel, PhD, a professor at the Yale School of Public Health and the senior author of a new paper projecting how U.S. foreign aid budget variations would affect the HIV epidemic in sub-Saharan Africa, offers a particularly cynical take on the new document outlining PEPFAR’s plans.
“It’s a ‘feel good, look at all we’re doing, we’re going to stop the epidemic in its tracks’ document,” Paltiel quipped.
Ever fine-tuning the approach:
To measure progress in combating HIV in sub-Saharan African nations and to look for key areas where the agency can hone its efforts, PEPFAR has in recent years funded the launch of a series of highly accurate surveys of the epidemics in an expanding roster of countries. Called a Population-based HIV Impact Assessment (PHIA), this survey method takes a massive, nationally representative sample through door-to-door household visits. The resulting rich data set allows researchers to make precise estimates of epidemic trends, breaking them down by key demographics, without having to rely on mathematical modeling.
Since December 2016, PHIA results from a six sub-Saharan nations with very high HIV prevalence rates have come in, stunning the public health community with their granular evidence of considerable success. Between 2011 and 2016, Swaziland saw its national viral suppression rate double, from 37 percent to 74 percent just as its annual infection rate plunged by nearly 50 percent.
In 2016, about 5,000 citizens with HIV died in Swaziland while 8,000 people contracted the virus. The agency’s goal is to drive down the infection rate to just 1,500 by 2020 (thus achieving epidemic control), a goal that appears achievable based on current trends. Pillars of PEPFAR’s plan to achieve this outcome include such measures as: expanding efforts to start people on ARVs the day they test positive for HIV; providing routine viral load testing nationwide to monitor medication adherence and the emergence of drug resistance; saving resources by reducing medical monitoring to only twice yearly for those doing well on HIV treatment; better targeting testing services where they are most needed; and trying out a self-HIV-testing program.

The annual rate of new HIV infections and deaths in Swaziland, projected forward to 2020. PEPFAR hopes to drive the infection rate below the death rate by 2019, achieving epidemic control.PEPFAR
The PHIAs conducted in Malawi, Zambia and Zimbabwe, where 10 percent to 15 percent of the national populations are living with HIV, have indicated that these nations have respective viral suppression rates of 68 percent, 60 percent and 60 percent. And in September, PEPFAR announced that Lesotho’s corresponding rate is 67 percent while Uganda’s lags behind at 48 percent.

The denominator changes in each progressive steps of these bar graphs. So in Swaziland, 85% of their HIV population is diagnosed, 87% of that group is on ARVs and 92% of that group is virally suppressed, for an overall viral suppression rate of 68%.PEPFAR
“I never expected it to be that good,” Jessica Justman, MD, an associate professor of medicine in epidemiology at the Columbia Mailman School of Public Health, says of the 60 percent–plus viral suppression rates in those five nations. “I thought it was going to be barely 50. And to be so close to that 73 percent number, that tipping point, I think it’s fantastic. I’m not ready to say we’re at the endgame with HIV. But you can kind of see where it might go. And that it’s going to require persistence and strength.”
Justman is the senior technical director at ICAP, Columbia’s global health organization. PEPFAR funds ICAP through the CDC fund to implement the PHIA studies in Africa in partnership with the CDC and other groups.

Columbia University’s Jessica Justman, discussing PHIA findings in an address at the 9th International AIDS Society Conference on HIV Science in Paris in July 2017.Benjamin Ryan
PEPFAR’s plan is to conduct PHIA studies on a rolling basis through 2019 in the remaining seven African countries on the list of 13 priority nations. Justman predicts that such surveys may not focus on the population as a whole but on more targeted demographics, such as the young.
Indeed, PEPFAR’s work in the 13 primary-focus nations will seek to better address the needs of men younger than 35—PHIA results have clearly spelled out this area for improvement—whose low viral suppression rate fuels HIV transmission among women ages 15 to 24 in particular. The agency will also ramp up a successful program called DREAMS that targets young women and will continue to expand programs that provide voluntary medical male circumcision (VMMC) among boys and young men. VMMC is associated with about a 60 percent reduction in female-to-male transmission of HIV according to a trio of major studies.
The budget:
In the spring, Trump’s proposed PEPFAR budget for the 2018 fiscal year called for a 17 percent cut, from $4.6 billion to $3.8 billion—this after years of flat funding despite expanding global need for HIV services. The president also sought a 19 percent cut (from $1.35 billion to $1.1 billion) to The Global Fund to Fight AIDS, Tuberculosis and Malaria and a 23 percent reduction in the budget for the National Institutes of Health (NIH), which drives much of the world’s most important HIV research.
Two studies, one presented in July at the 9th International AIDS Society Conference on HIV Science (IAS 2017) in Paris and the other subsequently published in the Annals of Internal Medicine, recently emerged detailing the devastation that U.S. foreign aid budget cuts could bring to people living with and at risk for HIV in sub-Saharan Africa in particular: namely, resurgent infection and AIDS-related death rates. The published paper found that budget cuts between 10 percent and 20 percent to HIV aid in South Africa would save the U.S. government just $900 for every year of life lost. (Economic analyses concerning the U.S. health care system often use $100,000 per year of life gained as the threshold below which a health intervention for Americans is considered cost effective.)
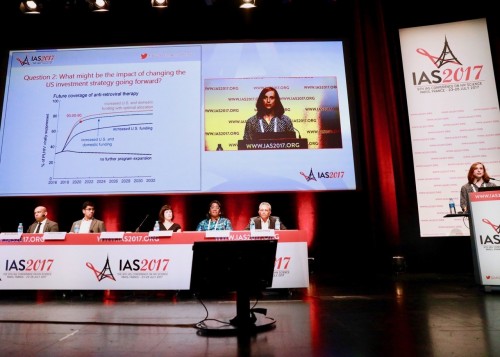
Jessica McGillen, PhD, presents a key slide at IAS 2017 in Paris that projects the impact of U.S. funding on viral suppression rates in 18 sub-Saharan African nations.Courtesy of Benjamin Ryan
Taking an apparent stand against the president, Congress has actually sought an increase in the NIH’s budget. Additionally, the Senate Appropriations Committee voted in September to maintain PEPFAR funding at about $6 billion. Although the two studies of the effects of future HIV aid budgets both project that flat funding would cause viral suppression rates to stagnate, PEPFAR nevertheless pledges to stick with its plan for expanded HIV treatment the 13 target nations as it waits for final word from Congress about its budget for next year.
“The Trump Administration remains deeply committed to the global HIV/AIDS response and to demonstrating clear outcomes and impact for every U.S. dollar spent,” Tillerson wrote in his introduction to the new PEPFAR plan.
During the IAS 2017 conference, Deborah L. Birx, MD, the Obama-appointed U.S. global AIDS coordinator and head of PEPFAR, repeatedly stressed how she was prepared to meet such business-minded demands for efficiency.
Some HIV advocates bristle at the mention of efficiency in the context of foreign HIV aid, worried that the word is a euphemism for cutting corners. On the contrary, to hear Birx describe the significance of the term as it applies to her agency’s work leaves the impression that PEPFAR intends to spend taxpayer dollars more effectively, allowing room for expansion with the same amount of money, instead of reducing the agency’s impact.

Ambassador Deborah Birx, the US Global AIDS Coordinator and Director of PEPFAR at IAS 2017Benjamin Ryan
The PHIA studies are a key driver of this quest for greater efficiency, providing the kind of precise demographic data that can help craft strategies to get a bigger bang for the buck. When analyzing the survey results, Justman says investigators are “looking to see where there’s a mismatch” between efforts to control the epidemic and successful outcomes.
“Nobody wants to spend money on something that’s a waste,” Justman says. “Nobody wants to work on something that’s not productive.”
Then there is the actual cost of ARVs, a major chunk of the PEPFAR budget. On this front, good news recently broke: Generic manufacturers have agreed to produce a fixed-dose, single-tablet ARV regimen based on Tivicay (dolutegravir) for no more than $75 per year in 92 poorer nations.
Tivicay, an integrase inhibitor commonly used in wealthier nations, has a particularly high barrier to the development of HIV drug resistance and a low side effect profile. The World Health Organization has proposed the ARV’s expanded use as an answer to the troubling worldwide rise of resistant virus. The tablet also includes generic versions of Epivir (lamivudine) and Viread (tenofovir disoproxil fumarate).
The global gag rule’s compromising effects:
PEPFAR’s work, however adequately funded and well intentioned, may be stymied by the Trump administration’s return to the so-called global gag rule, which prohibits the use of U.S. funds to support organizations that use funds from other sources to provide abortion services. The rule forbids even mentioning abortion as an option to women. Instituted by the Reagan administration in 1984, this foreign-aid policy has become a political shuttlecock in the decades since, with each subsequent new Democratic administration rescinding it and each new Republican presidency putting it back in place.
Trump has gone even further than George W. Bush in his approach to this policy. The Bush administration exempted PEPFAR from the gag rule over concerns that it would stymie HIV treatment and prevention efforts. Research ultimately backed up this move, with findings that the gag rule had greatly compromised HIV testing and condom distribution programs abroad. Trump has provided no such cover, expanding the rule to apply to nearly all global health efforts, from malaria to water sanitation and including HIV.

George W. BushNorthfoto/Shutterstock.com
“So it’s really a global gag rule on steroids,” says Serra Sippel, president of the Center for Health and Gender Equity (CHANGE) in Washington, DC.
Apparently, the gag rule isn’t even effective at its supposed goal of preventing abortions. Research out of Stanford University found that the George W. Bush–era gag rule was associated with a rise in abortion rates because it choked access to contraception.
Sippel says workers on the ground in Africa have reported that the gag rule will actually make the overall HIV fight less efficient by fracturing vital connections between health groups. For example, if family planning organizations in Africa refuse to excise abortion services from their operations and lose U.S. funding, this will likely hinder their ability to provide HIV testing services and, ultimately, referrals of newly diagnosed individuals to PEPFAR-sponsored treatment and care programs, including HIV-positive women in urgent need of ARVs to prevent transmission of the virus to their newborns.
As she praises PEPFAR, saying the agency is “making a difference and addressing the epidemic in a really smart way,” Sippel says of the gag rule, “There’s a sense of desperation, exasperation, that this is such an egregious policy. Lives are going to be lost.”
To read a POZ feature article on how HIV scientists are making significant progress in the glboal HIV fight, click here.
Editor’s note: A previous version of this article incorrectly stated that PHIA stands for a Public Health Impact Assessment, rather than a Population-based HIV Impact Assessment.
Benjamin Ryan is POZ’s editor at large, responsible for HIV science reporting. His work has also appeared in The New York Times, New York, The Nation, The Atlantic and The Marshall Project. Follow him on Facebook, Twitter and on his website, benryan.net.




Comments
Comments