
HIV cure researchers received some disappointing news at the July 2018 International AIDS Conference in Amsterdam. Two studies in particular offered a sobering lesson on how extraordinarily complex developing a safe and effective cure for the virus will likely be.
As conference attendees learned, researchers behind a randomized trial of an HIV cure method, the largest such study to date, recently found that their efforts failed to reduce viral DNA in human participants. The trial, called RIVER, tested the “kick and kill” strategy that seeks to roust latently infected immune cells from their slumber and then kill them off. Standard HIV medications—antiretrovirals, or ARVs—work only against cells that harbor actively replicating virus. These resting infected cells are a chief component of what is known as the viral reservoir, and it’s the stubborn persistence of this reservoir that frustrates cure efforts.
In a second study presented at the conference, an antibody treatment that had shown promise in monkeys failed to prompt what is known as posttreatment control of the virus after HIV-positive humans interrupted their ARV therapy.
As scientists in this field recalibrate their expectations, the use of the term “cure” as a goal for their research is declining. Instead, investigators may seek to induce posttreatment control of HIV, or viral remission, in which a particular therapy would not eradicate the virus from the body but rather suppress HIV over an extended period without the need for long-term ARV treatment.
Nevertheless, the overall field is generally still referred to as HIV cure research.
Taking the pulse of her fellow HIV cure researchers, Sharon R. Lewin, MD, PhD, director of The Peter Doherty Institute for Infection and Immunity at the University of Melbourne in Australia, says, “If anything, there was probably more optimism four years ago because we had tried fewer things. We now know that curing HIV is definitely not an easy task.”
Looking on the bright side, Lewin points to other promising recent cure studies conducted in primates, noting, “We definitely have been able to cure a few monkeys. That’s exciting.”
But as the antibody study presented at the Amsterdam conference indicated, disappointing outcomes among humans might follow success in primate research.
“The preclinical studies have universally shown more favorable outcomes than human studies,” says Jintanat Ananworanich, MD, PhD, who in her capacity as the associate director for therapeutics research at the U.S. Military HIV Research Program directs research in the HIV cure field. “Although no strategies have resulted in remission in clinical trials thus far, tremendous knowledge on HIV persistence and immune responses has been generated. This is important to informing future trials.”
Concerns about recent setbacks notwithstanding, Lewin remains optimistic about the future of HIV cure research. “Science can also take dramatic turns with significant discoveries too,” she says. “So you never know what may change the field dramatically.”
Lewin is the lead author of a literature review recently published in The Lancet HIV, “Barriers and Strategies to Achieve a Cure for HIV,” in which she and her three coauthors offer a comprehensive summary of the impressive number of avenues researchers are pursuing in their quest for a cure, or something close to it. Below, POZ looks at the main takeaways from their paper. We also explore a few HIV cure studies published more recently.
***
Lewin and her colleagues note that the only person ever cured of HIV remains Timothy Ray Brown. As a component of his treatment for leukemia, Brown received stem cell transplants a decade ago from a donor with a genetic mutation that confers natural resistance to the virus—the surface of the donor’s immune cells lacked the CCR5 coreceptor to which most HIV attaches in order to infect the cells. As far as researchers can tell, Brown benefited from a sterilizing cure. There is no evidence in his body of any virus with the capacity to replicate, and his viral load has never rebounded. (Today, Brown actually takes Truvada [tenofovir disoproxil fumarate/emtricitabine] as pre-exposure prophylaxis [PrEP] to ensure he does not contract HIV again.)
Otherwise, in the realm of posttreatment control of HIV, quite a few people with the virus have been able to suppress their viral load for long stretches, sometimes for years, after interrupting standard ARV treatment. A recently published paper found that those who began ARVs very soon after contracting the virus are more likely to achieve such a prolonged state of viral remission after eventually going off their meds. It is likely that beginning on ARVs so promptly after infection keeps the viral reservoir relatively small, thus reducing the likelihood of latently infected cells springing to life at any given moment following a treatment interruption.
One of the most famous cases of such posttreatment control is that of the African child who was treated for HIV for less than a year after birth and, by the time the child’s case was reported in 2017, had spent over eight years in a state of viral remission. In 2015, news surfaced that an 18-year-old French individual had spent 12 years off ARVs and still controlled the virus. Then, of course, there was the 2013 case of “the Mississippi Child”—met with great fanfare—who spent a couple of years off ARVs during her very young life but ultimately, and disappointingly, experienced a viral rebound at 4 years old.
According to Lewin, scientists’ increasingly enriched comprehension of the posttreatment-control phenomenon has actually made designing HIV cure studies more difficult. Now researchers must take into account that some study participants might achieve control of their virus, even if for a short time, without the benefit of an investigative cure therapy, thus making it more challenging to prove that a cure treatment was the cause of viral remission or a delayed viral rebound after the interruption of ARV treatment.
***
Not only do latently infected immune cells evade ARV treatment, but also for every million such cells, perhaps only 60 harbor virus that can actually replicate; the rest contain defective virus. So finding those resting cells capable of waking up and repopulating the body with new virus in the absence of ARV treatment can be akin to finding a needle in a haystack. The immune system itself wastes considerable energy going after cells infected with dud copies of the virus.
In another of the myriad ways HIV has evolved to help ensure it sustains a lifelong infection, latently infected cells have the ability to clone themselves. Perhaps more than half of the viral reservoir cells in some people living with the virus are clones.
The matter of whether HIV continues to replicate at low levels in the face of effective ARV treatment has been the source of significant controversy in the cure field. A study presented at the 2018 Conference on Retroviruses and Opportunistic Infections in Boston found no evidence of such ongoing replication in the lymph nodes, calling into question the notable contrasting findings of a 2016 paper.
***
The lack of precise tests for measuring the viral reservoir remains a considerable obstacle for HIV researchers, both in determining the challenge they face in their quest to vanquish an infection and in assessing how well they did. Currently, scientists in the field must rely on rather crude metrics, such as changes in the overall presence of viral DNA or RNA in the blood, to gauge how a particular treatment affects the size of the reservoir. (HIV carries its genetic code in RNA, which is copied to DNA during infection of a cell.) Such metrics can underestimate the population of infected cells because most virus hides in tissues, not blood.
Scientists may also try to measure success by determining whether an HIV cure treatment is associated with a delay in viral rebound after an interruption of ARV therapy and whether such a treatment is associated with a particular level of control of the virus in the absence of standard ARV therapy for the virus.
If only scientists could identify a specific biomarker, such as a particular protein, that could predict the likelihood of a delay to viral rebound or control of the virus after a treatment interruption. Then, study participants might be spared the burden of interrupting their ARVs, a common requirement in HIV cure study designs. Asking people to stop standard HIV treatment raises ethical questions and may discourage people living with the virus from entering cure trials. That said, multiple studies have indicated that treatment interruptions in cure studies are safe.
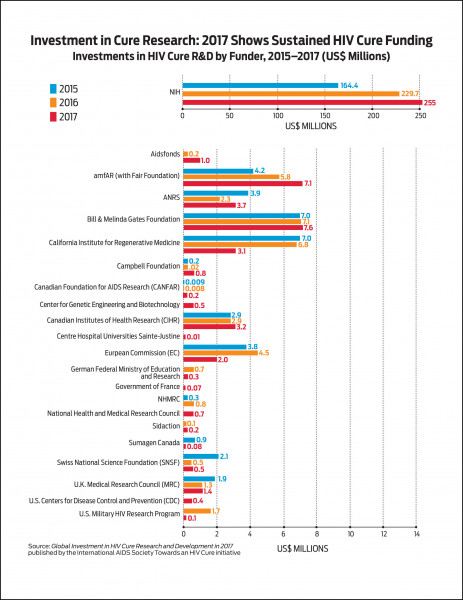
Lewin argues that such a tidy biomarker would likely attract greater investment in the field from pharmaceutical companies. (Global funding for public sector HIV cure research increased from $88 million in 2012 to $289 million in 2017, with the lion’s share coming from the National Institutes of Health.) Such for-profit companies prefer study designs boasting a level of simplicity that will help an investigational treatment pass muster with regulatory bodies like the Food and Drug Administration. They also prefer efficient investments for their research and development dollars. So their researchers favor clearly delineated, objective means of measuring success in clinical trials of experimental agents.
Case in point: The recent discovery of a biomarker that can predict whether an individual will achieve a functional cure of hepatitis B virus (HBV) gave rise to a surge of interest from the pharmaceutical industry in researching curative therapies for HBV.

Source: “Global Investment in HIV Cure Research and Development in 2017”
Source: “Global Investment in HIV Cure Research and Development in 2017”
Avenues of Research:
Stem cell transplants
Clinicians are still trying to replicate the success of Timothy Brown’s HIV cure with similar strategies. In recent years, a number of other individuals with cancer have received stem cell transplants from donors who also have the genetic mutation related to the CCR5 coreceptor that confers resistance to the virus. One of the six such individuals whose cases have been published in scientific literature experienced a viral rebound; the other five ultimately died as a result of complications following their stem cell transplant or from their underlying cancer.
In other cases of people living with HIV who received a stem cell transplant but from a donor who lacked the CCR5-related genetic mutation, the stem cell transplant did delay the time to viral rebound by 3 to 10 months after the individuals stopped ARVs.
However, the high fatality rate following transplantation highlights how impractical, not to mention unethical, this method of attempting to cure HIV is for anyone not already facing a high risk of death due to cancer.
Gene therapy
Seeking safer alternatives to cancer-treatment-based stem cell transplants, researchers are experimenting with gene-editing techniques that alter the DNA of an individual’s immune cells. In particular, the scientists will try to deactivate the gene that gives rise to the CCR5 coreceptor, thus robbing HIV of a means of latching onto immune cells. The modified cells are then grown outside the body and ultimately reinfused into the person’s body. The aim is to spawn a population of immune cells that are resistant to infection. As the field of gene editing rapidly evolves, it is hoped that new, even more cutting-edge technology will facilitate progress on the HIV cure front.
“Kick and kill”
The method of waking up latently infected cells (the “kick” part) and then finishing them off (the “kill” part) has yielded some notably disappointing results of late, including those of the RIVER study that was presented at the July conference in Amsterdam. Researchers pursuing this strategy have looked to various cancer drugs known as HDAC inhibitors as the kick element; but thus far, they have not been able to show such drugs can actually diminish reservoir cells.
Lewin remains cautiously optimistic about further research into these medications, noting that the RIVER trial used a less advanced and relatively weak kick agent. Recent, more preliminary studies that have examined other kick agents, such as so-called TLR agonists, have shown far greater promise.
On this front, Gilead Sciences is investigating a drug known as GS-9620 that has shown positive results in primate research.
Latency silencing: “block and lock”
Effectively the opposite of the kick and kill strategy, the “block and lock” method, also known as latency silencing, is based on the presumption that if rooting out and killing all the latently infected cells in the body is too challenging, keeping them in a silent state indefinitely may be a viable alternative. A recent study conducted in mice sought to inhibit a viral protein known as tat that acts as an on-off switch for viral replication in cells. The study successfully reduced the amount of HIV RNA expressed in tissue biopsies taken from the animals, and it delayed viral rebound after the interruption of ARV treatment.
Enhancing the immune system
Researchers are investigating whether vaccines can be used to prompt the body to better control the virus.
Scientists have also invested considerable energy into studying so-called broadly neutralizing antibodies, which are natural antibodies that boast the capacity to combat a wide array of HIV strains. Research has indicated that some of these antibodies are associated with a delay in viral rebound after an ARV treatment interruption. Recently, scientists have gone high-tech by synthesizing three such antibodies into one “trispecific” antibody—a kind of all-in-one triple combination therapy—that has already shown promise in its use as pre-exposure prophylaxis (PrEP) among primates.
Modulating the immune system
Scientists are seeking to manipulate proteins that redirect the traffic of immune-fighting cells. One such example is an antibody called vedolizumab that targets a protein on the surface of CD4 cells and stops these cells from moving into the gut, where HIV focuses much of its assault on the immune system. An initial study in monkeys reported two years ago provided hope for progress in this area of research, but scientists recently repeated the study and found that the antibody had a null impact on the second go-round. Preliminary results in humans also showed that vedolizumab did not affect the time to viral rebound after individuals interrupted their ARV treatment.
Looking to the future
In all likelihood, a successful HIV cure, or posttreatment control, strategy will rely upon a combination approach based on a number of the methods currently under investigation or those yet to be imagined.
“It is clear that achieving HIV remission will not be easy and that one should not expect any single intervention to help people get to remission,” says Jintanat Ananworanich. “We are taking small steps in discovery science.”
Any successful method will need to be safe, effective and—if it is to make a significant dent in the global epidemic—scalable. An HIV cure therapy that is extraordinarily expensive thanks to, for example, the highly involved and complex process required to provide personally tailored genetic editing of an individual’s immune cells, will have little to offer poorer nations—in particular those in sub-Saharan Africa—where the need is greatest.
Curative hepatitis C virus (HCV) treatment, for example, costs tens of thousands of dollars in the United States, which has led insurers to restrict coverage of the medications. The actual cost to manufacture such medications, however, is relatively low, which allows for a steep sliding scale elsewhere around the world.
The future of HIV cure science is also up against the phenomenal success of ARV treatment, which has set a high bar for any alternative means of suppressing the virus. The life expectancy of those on ARVs is approaching normal. What’s more, the risk of transmitting HIV is effectively zero for those who maintain a fully suppressed viral load.
However, such benefits don’t speak to the psychic costs of living with a highly stigmatized lifelong infection or how a cure therapy may alleviate such burdens. Then there are the extreme difficulty and expense of getting the global population on lifelong ARV treatment. Also, even well-treated HIV is associated with an increased risk of numerous health conditions, such as cardiovascular disease and cognitive decline.
Some form of HIV cure could help address these problems. However, as HIV drug development continues to progress and long-acting injectable treatments, or even very long-lasting implants, become the standard of care, emerging HIV cure treatments may cease to offer the freedom from daily medications as an advantage over standard ARV therapy. (Or perhaps by then, long-acting antibody treatments will be the norm.)
Furthermore, if someone is in a state of posttreatment control of the virus, what reassurances will there be that the virus will remain dormant indefinitely and won’t suddenly surge back and make an individual unwittingly infectious? How frequently will people benefiting from viral remission need viral load monitoring?
These pressing questions, along with HIV’s extraordinary complexity, likely make for a long and winding scientific road ahead. But thanks to the increasing funds backing such research and a growing army of top-tier scientists doggedly pursuing a cure, the future will hopefully prove bright with new developments.
Still, this field isn’t simply concerned with a binary outcome of finding the holy grail of a cure or otherwise failing to do so. Success will likely prove incremental, with scientists eventually discovering new means of further mitigating HIV’s long-term harms, further transforming a once surely fatal infection into an increasingly innocuous presence in the body and around the world.




3 Comments
3 Comments